Chronically elevated blood glucose triggers a cascade of molecular injuries — oxidative stress, protein glycation, mitochondrial overload, and ultimately organ failure. This page traces that damage step by step, including Dr. Jason Fung's two-phase model of how sugar causes Type 2 Diabetes.
When blood glucose remains persistently elevated — a condition known as hyperglycemia — cells throughout the body suffer a cascade of molecular injuries[1]. The damage spans from individual proteins and organelles all the way up to entire organs. Here is how it unfolds.
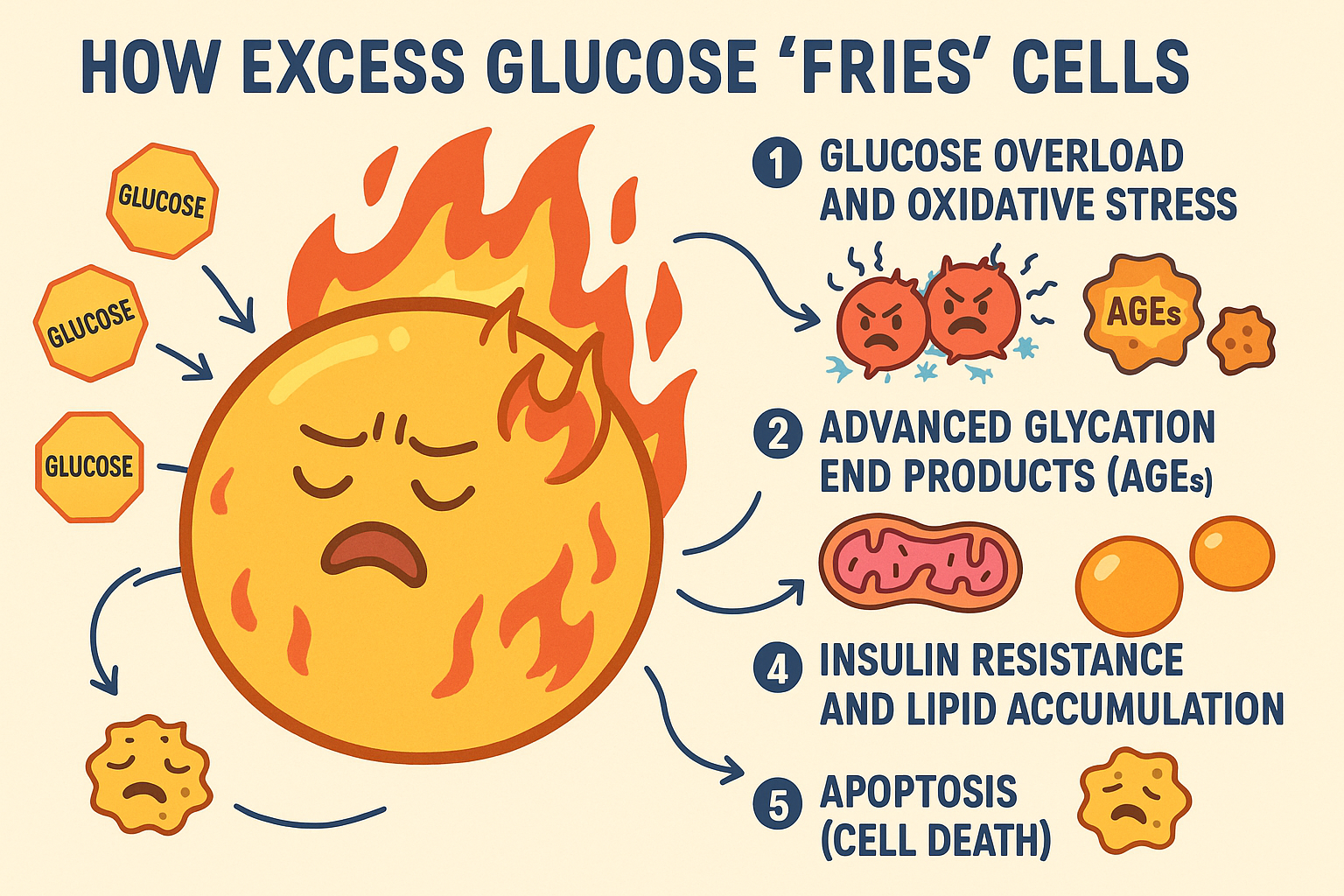
Glucose Overload & Oxidative Stress
When cells are overwhelmed with glucose, the electron transport chain in mitochondria receives far more substrate than it can process cleanly. Electrons "leak" off the chain and combine with oxygen to form reactive oxygen species (ROS) — unstable free radicals that attack DNA, membrane lipids, and structural proteins.[2]
This oxidative stress is the master trigger behind most of the downstream complications of chronic hyperglycemia, including neuropathy, retinopathy, and cardiovascular damage.
Advanced Glycation End Products (AGEs)
Excess glucose reacts spontaneously with proteins and fats in a process called non-enzymatic glycation. The resulting molecules — AGEs — are chemically altered structures that the body cannot repair normally.[3]
- Stiffen collagen in blood-vessel walls, raising blood pressure
- Activate inflammatory signaling through the RAGE receptor
- Damage kidney filtration membranes (diabetic nephropathy)
- Cloud the lens of the eye (diabetic cataracts)
AGE accumulation is a major reason why years of elevated blood sugar translate into structural damage that cannot simply be reversed by lowering glucose later.
Mitochondrial Overload
Muscle cells, neurons, and heart cells are energetically demanding and rely heavily on mitochondria. Too much glucose floods the citric-acid cycle and electron transport chain, causing the mitochondria to:[4]
- Leak electrons, generating excess ROS (see diagram)
- Lose membrane potential — reducing ATP yield
- Fragment their inner membrane (cristae), impairing function
- Trigger mitochondrial apoptosis pathways
The analogy is an engine running on too much fuel with a clogged exhaust — the heat and backpressure damage the engine itself.
Insulin Resistance & Lipid Accumulation
Chronically high glucose drives the pancreas to secrete more and more insulin. Over time, cells become desensitized — a state called insulin resistance.[5]With glucose unable to enter cells efficiently, blood sugar stays elevated, and the liver converts the excess into fat:
Fat accumulates in non-fat tissues — the liver and skeletal muscle in particular. This lipotoxicity amplifies inflammation, disrupts intracellular signaling, and accelerates cell death. It also creates a vicious cycle: fat in the liver worsens insulin resistance, which raises glucose further.
The Two-Phase Model — Dr. Jason Fung
In The Diabetes Code[7], Dr. Jason Fung synthesizes research by Roy Taylor[8][9] into a compelling two-phase explanation of how chronic sugar consumption progresses to Type 2 Diabetes:
Phase 1 — Fatty Liver: Years of high sugar intake overflow the liver's glycogen stores. The liver converts the surplus into fat (de novo lipogenesis), which accumulates within liver cells. This fatty liver is the first organ to become insulin resistant, forcing the pancreas to compensate with ever-higher insulin secretion.
Phase 2 — Fatty Pancreas: When the liver becomes too saturated with fat, it begins exporting fat into the bloodstream (as VLDL). This fat deposits in the pancreas, directly poisoning the insulin-producing β-cells. Once β-cell function collapses, the body can no longer control blood glucose — Type 2 Diabetes has arrived.
The hopeful implication: because fat accumulation is the cause, dramatic caloric restriction or fasting can reverse both stages — restoring β-cell function and resolving diabetes in many patients.
Apoptosis — Programmed Cell Death
When oxidative stress, mitochondrial dysfunction, and toxic fat accumulation persist long enough, cells activate apoptosis — a controlled self-destruction program designed to contain damage.[6] The cell packages its contents into membrane-bound fragments (apoptotic bodies) that neighboring immune cells clear away.
In the pancreas this is catastrophic: β-cells lost to apoptosis are not replaced. In nerves (peripheral neuropathy) and retinal cells (retinopathy) the same irreversible loss occurs — explaining why diabetic complications are easier to prevent than to reverse.
Why "Fried"? — The Unifying Analogy
Dr. Fung's "fried" metaphor captures the mechanism precisely. Just as food burns when exposed to excess heat or oil, cells are damaged when flooded with excess fuel:
- Oxidative stress (ROS) = the heat that chars the surface
- AGEs = the caramelization that stiffens and discolors proteins
- Mitochondrial burnout = the engine overheating from too much fuel
- Fatty liver → fatty pancreas = the oil that eventually destroys the pan
The "burning" is not literal — it is oxidative and metabolic damage. But the result is the same: a cell that can no longer function normally.
References
- Nakrani MN, Wineland RH, Anjum F (2023). Physiology, Glucose Metabolism. StatPearls (NCBI Bookshelf). https://www.ncbi.nlm.nih.gov/books/NBK560599/
- Brownlee M (2005). The Pathobiology of Diabetic Complications: A Unifying Mechanism. Diabetes. https://pubmed.ncbi.nlm.nih.gov/15919781/
- Twarda-Clapa A, Olczak A, Białkowska AM, Koziołkiewicz M (2022). Advanced Glycation End-Products (AGEs): Formation, Chemistry, Classification, Receptors, and Diseases Related to AGEs. Cells. https://pmc.ncbi.nlm.nih.gov/articles/PMC9139786/
- Bhatt MP, Ha HC, Kim YM, Ha KS (2022). Diabetic Conditions Promote the Loss of the Blood–Brain Barrier Integrity through Mitochondrial Dysfunction. International Journal of Molecular Sciences. https://pmc.ncbi.nlm.nih.gov/articles/PMC8910741/
- Freeman AM, Acevedo LA, Pennings N (2023). Insulin Resistance. StatPearls (NCBI Bookshelf). https://www.ncbi.nlm.nih.gov/books/NBK507839/
- Fiorentino TV, Prioletta A, Zuo P, Folli F (2013). Hyperglycemia-induced oxidative stress and its role in diabetes mellitus related cardiovascular diseases. Current Pharmaceutical Design. https://pubmed.ncbi.nlm.nih.gov/23127236/
- Fung J (2018). The Diabetes Code: Prevent and Reverse Type 2 Diabetes Naturally. Greystone Books. https://www.greystonebooks.com/products/the-diabetes-code
- Taylor R (2008). Pathogenesis of type 2 diabetes: tracing the reverse route from cure to cause. Diabetologia. https://pubmed.ncbi.nlm.nih.gov/18726069/
- Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ, Mathers JC, Taylor R (2011). Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia. https://pubmed.ncbi.nlm.nih.gov/21656330/